
Paid Advertiser
Paid Advertiser
Model of care
Strategies for treating early relapse of multiple myeloma


Paid Advertiser
Paid Advertiser
Multiple myeloma (MM) is a disease frequently characterized by repeated cycles of remission and relapse. Advances in upfront treatment of MM have prolonged remission intervals, though many patients still experience first relapse within several years of diagnosis.1
“Early detection of relapse is important because it allows you to make more informed decisions and have more options,” explains Joshua Richter, MD, Associate Professor in the Icahn School of Medicine at Mount Sinai. “You’re always going to make better decisions if you don’t have to do it under duress.”
Failure to detect relapse early can lead to more severe complications from disease, which can complicate treatment decision-making. “It may mean you have to give them something more aggressive so that they respond quicker,” Dr. Richter says. “More aggressive may mean more side effects.”
The bottom line: “Having insight into the progression process earlier on gives you a more broad-based platform to pick a more optimal therapy,” Dr. Richter says.
Monitoring and detection
In most cases, early relapse is detected during regular monitoring. Depending on the type of frontline treatment and maintenance therapy the patient received, as well as their disease characteristics, testing may be done every 1 to 3 months. Myeloma labs may include a variety of blood and urine tests, such as:2
- a complete blood count
- blood chemistry panels
- serum (SPEP) and urine protein electrophoresis (UPEP)
- quantitative immunoglobulins
- a serum-free light chain assay
Carol Ann Huff, MD, Associate Professor of Oncology and Medical Director for the Johns Hopkins Kimmel Cancer Center, notes that symptoms such as pain or fatigue may serve as warning signs of early relapse as well, though most cases are detected on bloodwork.
Treatment decision-making:
factors to consider
“Myeloma doesn’t have clear-cut guidelines in early relapse,” notes Dr. Richter. A variety of treatment options is available within the early relapse setting—that is, for patients with 1 to 3 prior lines of therapy.3 “We usually incorporate three dimensions of characteristics into picking a treatment: patient-related factors, disease-related factors and treatment-related factors,” says Dr. Richter. For example:
- Patient-related factors include considerations such as age, frailty and the presence of certain comorbidities, such as renal impairment.
- Disease-related factors that affect treatment decision-making include how fast the myeloma is progressing as well as the presence of high-risk genetic markers or extramedullary disease.
- A variety of treatment-related factors affects approaches to subsequent lines of therapy. These include not only the efficacy and safety of treatment options but also the patient’s treatment history—how well they have responded to previous therapies, side effects that were experienced and whether patients have developed refractory disease to early treatment regimens.3 Practical considerations should be weighed as well, including costs, scheduling and overall impact on quality of life.
“Having insight into the progression process earlier on gives you a more broad-based platform to pick a more optimal therapy.”
Anti-CD38 monoclonal antibodies in early relapse
Anti-CD38 monoclonal antibodies (mAbs) have emerged as integral components of early relapse treatment approaches.3 “One of the things we started to realize was that anti-CD38 drugs, like daratumumab and isatuximab, really function optimally as part of an upfront strategy and/or as part of an early-relapse strategy,” explains Dr. Richter.
Guidelines from the National Comprehensive Cancer Network (NCCN) list daratumumab-based combination therapy as an option for primary treatment of both transplant-eligible and -ineligible patients.3 As a result, Dr. Richter notes that an increasing number of patients are entering first relapse anti-CD38-exposed. “As long as they’re not refractory to it, and most people are not refractory to an anti-CD38 going into early relapse, we recommend incorporating an anti-CD38 as part of your early relapse strategy,” he says.
Choosing an anti-CD38-based regimen
“One of the things we started to realize was, pound for pound, anti-CD38s plus carfilzomib are more efficacious regimens than anti-CD38s plus pomalidomide,” notes Dr. Richter. Within the NCCN guidelines, carfilzomib in combination with either daratumumab or isatuximab (and dexamethasone) is considered a preferred early-relapse regimen, particularly for those with bortezomib- or lenalidomide-refractory disease.3
“So for the patients we worry about the most—the high risk, the functionally high risk (early relapse), those with extramedullary disease—we tend to give an anti-CD38 plus carfilzomib,” says Dr. Huff. “And although we can never compare trial to trial, if you look at the early relapse data, the best data to date are the IKEMA data.”
The IKEMA trial: unprecedented progression-free survival
The IKEMA phase 3 clinical trial evaluated the efficacy and safety of isatuximab in combination with carfilzomib and dexamethasone (Isa-Kd) in patients with 1 to 3 prior lines of therapy. Updated results from the IKEMA trial were published in May 2023, which demonstrated a median progression-free survival (PFS) of 35.7 months after a median 44 months of follow-up, as evaluated by an Independent Response Committee.4 Further analysis following the FDA recommendations on censoring rules showed a median PFS of 41.7 months.
“That is an absolutely incredible number,” emphasizes Dr. Richter. “And it’s available everywhere—community, academic, you name it—and it doesn’t require any special technology.” Dr. Richter adds that for many patients, particularly those with significant cardiac disease, use of carfilzomib may be more complicated or contraindicated. In these cases, an anti-CD38-based regimen plus pomalidomide may be preferred.
Selecting an anti-CD38 mAb
Both Dr. Richter and Dr. Huff note that isatuximab and daratumumab are highly active and efficacious therapies that are well-tolerated in early relapse of MM. Dr. Richter says that for patients who responded well to daratumumab as primary treatment, there is a strong likelihood that the drug will work again. However, if patients have received another line of therapy since daratumumab, he notes he may elect to treat with isatuximab instead.
“For people who have progressed on daratumumab in an early setting, if they’ve had a chance to repopulate their CD38 expression (typically 4 to 6 months), I consider using isatuximab in the relapse setting,” says Dr. Richter.
Dr. Huff and Dr. Richter also note that there is emerging evidence to suggest that patients with a gain of chromosome 1q—typically considered a poor prognostic marker in MM—may respond to isatuximab treatment.5
In a subgroup analysis of the IKEMA and ICARIA-MM trials—the latter of which investigated the use of isatuximab in combination with pomalidomide and dexamethasone (Isa-Pd)—PFS was improved in isatuximab-treated patients with 1q gain mutations (1q21+) compared with patients who received Pd or Kd alone.6 Based on these results, one may consider isatuximab over daratumumab in combination with carfilzomib or pomalidomide in this situation.
Two key considerations for optimal treatment
First, Dr. Huff emphasizes that treatment within the early relapse setting of MM should be a collaborative process with both patients and family members. “Decision-making is shared,” Dr. Huff emphasizes. All discussions should incorporate insights from both the healthcare team and patient as well as family members involved in care.
And the second: “Try to use three-drug combinations as long as possible, substituting at least one new agent—two if high-risk early relapse,” she added. “Employ the regimen with the greatest probability for longest duration of remission while taking all other factors into consideration.”
—by Morgan Meissner
“Employ the regimen with the greatest probability for longest duration of remission while taking all other factors into consideration.”
References
1. Rajkumar SV, Kumar S. Multiple myeloma current treatment algorithms. Blood Cancer J. Sep 28 2020;10(9):94. doi:10.1038/s41408-020-00359-2
2. American Cancer Society. Tests to find multiple myeloma. Updated February 28, 2018. Available at cancer.org.
3. National Comprehensive Cancer Network. NCCN guidelines: multiple myeloma, version 3.2023. Updated December 8, 2022.
4. Martin T, Dimopoulos MA, Mikhael J, et al. Isatuximab, carfilzomib, and dexamethasone in patients with relapsed multiple myeloma: updated results from IKEMA, a randomized Phase 3 study. Blood Cancer J. May 9 2023;13(1):72.
5. Schmidt TM, Fonseca R, Usmani SZ. Chromosome 1q21 abnormalities in multiple myeloma. Blood Cancer J. Apr 29 2021;11(4):83.
6. Martin T, Richardson PG, Facon T, et al. Primary outcomes by 1q21+ status for isatuximab-treated patients with relapsed/refractory multiple myeloma: subgroup analyses from ICARIA-MM and IKEMA. Haematologica. Oct 1 2022;107(10):2485-2491.
Practice Pearls
Adjunctive therapies to manage complications and side effects


Paid Advertiser
Paid Advertiser
Treatment of multiple myeloma (MM) is based not only on the use of cancer-directed therapies but also on the incorporation of adjunctive treatments. Many organ systems are affected by MM, and the effects of the disease on the body can create a variety of bothersome symptoms and potentially dangerous complications.
Additionally, as patients with MM are exposed to a growing number of lines of treatment—and for longer durations with maintenance therapy regimens—management increasingly requires healthcare professionals to address various treatment-related side effects.
“It’s important to educate patients and set realistic expectations,” says Carol Ann Huff, MD, Associate Professor of Oncology andMedical Director for the Johns Hopkins Kimmel Cancer Center. “Then offer support and adjustment as needed.” Here are some of the most common disease symptoms, complications and drug side effects as well as how to address them.
Bone damage
This complication of MM is caused by the destruction and crowding out of healthy bone marrow cells by myeloma cells. As a result, bone pain is among the most common presenting symptoms of myeloma, and more than 80% of patients will develop bone complications over the course of disease.1 These include bone fracture as well as hypercalcemia and spinal cord compression.
In addition, certain anticancer therapies, such as steroids, can lead to weakening of the bones and may contribute to progression of bone disease.2 Patients also may have comorbid conditions that place them at risk for poor bone health, including osteoporosis, metastatic malignancies, immobility and side effects from long-term steroid and other drug use. Plus, certain factors can contribute to osteoporosis, including renal disease, hormonal changes, depression and diabetes as well as vitamin D and other vitamin/mineral deficiencies.
Management of bone disease in MM is typically based on the use of bisphosphonates such as zoledronic acid and pamidronate, as well as RANK-L inhibitors such as denosumab. While these drugs can help slow and even reverse the progression of bone disease, they can lead to osteonecrosis, most notably osteonecrosis of the jaw (ONJ), a rare but serious side effect that can be seen with prolonged use of bisphosphonates.2
Risk for ONJ can be mitigated by reducing the frequency of treatment and by avoiding invasive jaw procedures such as dental extractions and implants during treatment. All other dental procedures, including regular cleanings, fillings, root canals and crowns, should be performed as needed. Patients should be instructed to inform their dentist that they are receiving bisphosphonates or RANK-L inhibitors and encouraged to seek a second opinion from a dental specialist before receiving invasive dental procedures.
Pain medications such as narcotics may also be used to help manage bone pain. However, because MM can compromise the health of the kidneys, avoidance of nonsteroidal anti-inflammatory drugs is generally recommended.3 In cases of severe bone disease, surgery may be needed to address fractures and other related complications.
Neuropathy
Certain myeloma treatments can lead to nerve damage and peripheral neuropathy, which causes numbness, tingling or pain in the extremities. “Neuropathy can be problematic as there are not available therapies to treat this, only medications that may lessen the intensity of neuropathy symptoms,”says Dr. Huff. “Early intervention and prevention, where possible, are the best approaches.”
Neuropathy has been identified as a potential side effect of the immunomodulatory drug (IMiD) thalidomide (which is not frequently used in modern treatment plans), as well as the proteasome inhibitors bortezomib and ixazomib. The risk for peripheral neuropathy with bortezomib treatment can be lowered by using subcutaneous formulations and weekly dosing. Dr. Huff also suggests early intervention with dose reductions if possible if peripheral neuropathy occurs and careful questioning to identify early symptoms that may warrant dose adjustment or intervention.
“Some have found supplements helpful to lessen neuropathy, although clinical trials are lacking,” she notes. These include coenzyme Q10 (CoQ10), B vitamins and alpha lipoic acid. “Neuropathy that is painful is also sometimes helped with gabapentin, pregabalin or duloxetine.”
Blood effects
A variety of blood effects can be observed as a result of both MM and treatment, including anemia, thrombocytopenia and neutropenia, as well as thromboembolic disease. These effects can lead to other—potentially serious—complications as well, including bleeding, infection and fatigue. In addition, neutropenia and other blood effects are seen in patients treated with anti-CD38 monoclonal antibody-based regimens, IMiDs (lenalidomide and pomalidomide), proteasome inhibitors (bortezomib) and the nuclear export inhibitor selinexor.2,4 When patients are receiving IMiDs such as thalidomide, lenalidomide or pomalidomide, additional medications, including aspirin, low molecular weight heparin, warfarin or one of the newer direct anticoagulants, are often added to reduce the risk of blood clots.
Blood effects may be managed with dietary supplements (e.g., iron for anemia) as well as colony-stimulating factors. Preventative measures, including vaccinations, antibiotics, antivirals and, depending on the treatment regimen, antifungals and intravenous antibodies, may be administered to reduce the risk of infection due to neutropenia.
Gastrointestinal effects
A variety of MM treatments can cause gastrointestinal problems such as constipation, diarrhea, nausea and vomiting. Dr Huff notes that diarrhea is particularly a problem among people receiving long-term lenalidomide treatment. “For lenalidomide-associated diarrhea, use of bile acid-binding resins can help,” she says. “Cholestyramine or colesevelam are often more helpful than loperamide and other OTC antidiarrheals.”
Dr. Huff notes that constipation can also occur with steroid use as well as with the use of antiemetics such as ondansetron and certain pain medications. Stool softeners or laxatives can help relieve constipation, as well as a high-fiber diet, increased water intake and gentle exercise.
Sleep disturbances
Sleep problems such as insomnia are a common side effect associated with steroid use. Changes in sleeping patterns can also be indicative of nervous system effects associated with bispecific antibody therapies.2
“Sleep disturbances can be mitigated in some by changing the time of day of steroid administration, using sleeping medications, and with dose reductions of steroids where necessary,” says Dr. Huff. For example, she says, “Sometimes nighttime dosing helps as patients sleep through the first 6 to 8 hours.” She cautions that this approach will not work for all patients, though, and may not be possible depending on the requirements of treatment. At times, steroid dose reductions where medically appropriate may be needed. Melatonin or other sleep aids are of variable help.
Novel treatment-related side effects
Chimeric antigen receptor (CAR) T-cell therapies and bispecific antibodies represent new classes of drugs that have revolutionized MM treatment, particularly in later stages of disease. However, with these novel therapies has come a new set of rare but potentially serious side effects, including cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS). Use of these drugs requires prolonged monitoring to support early detection and rapid initiation of treatment within specialized centers.
—by Morgan Meissner
Nondrug interventions for managing myeloma symptoms
In addition to adjunctive medical treatments, it’s important to discuss nondrug therapies with patients, notes Shebli Atrash, MD, Assistant Professor of Clinical Medicine, Wake Forest Medical College, and multiple myeloma specialist at Atrium Health Levine Cancer Institute, Charlotte, NC. “Complementary and supportive therapies can significantly manage symptoms and improve the quality of life for individuals with multiple myeloma,” he says. Here, Dr. Atrash discusses some of the nondrug interventions that can help.
Q. What types of exercise do you recommend to patients and why?
A. Many myeloma therapies increase the risk of blood clots. Therefore, physical activity and exercise are advisable. Walking is the preferred physical activity because running or lifting weights could cause fractures in weak bones. Other good options include a stationary bike with low level of resistance or an elliptical machine. In general, there should be more focus on light exercises. I tell my patients, “The more you do, the better, but if you have muscle soreness the next day it means you overdid it.”
Q. Which complementary therapies might be helpful?
A. There are several options, but I’ll point out two of them. First, acupuncture appears to be promising and is currently undergoing investigation to explore its capabilities in the treatment of peripheral neuropathy, nausea and fatigue. Another thing that can help patients overall: engaging in creative activities to reduce stress. These activities—for example, journal writing, taking an art class or doing photography—can offer a sense of accomplishment and distraction from symptoms.
Q. What psychosocial interventions do you recommend?
A. The available support groups for multiple myeloma are exceptional because of the strength of support that families and friends have created. These can provide emotional support, a sense of community and a venue to share experiences and coping strategies. Patients can find them through the International Myeloma Foundation (myeloma.org), the Leukemia & Lymphoma Society (lls.org) and similar organizations.
Q. Are there any simple, everyday strategies that patients may find helpful?
A. Yes, and one of the most important is hydration. Myeloma progression is often complicated with dehydration symptoms. Staying hydrated can help manage symptoms such as fatigue and constipation and help protect the kidneys from myeloma injury.
In addition, muscle cramps remain a problem for patients on chemotherapy. Swallowing a teaspoon of mustard or an ounce of pickle juice might help decrease muscle cramps, as reported anecdotally by patients. It has not been determined why these may help. Some research speculates it could be because they contain acetic acid, which the body uses to produce acetylcholine, an essential neurotransmitter for leg muscle contractions. Yellow mustard is the only kind of mustard documented to relieve nighttime leg cramps, although more research is needed to confirm this.


References
1. Bernstein ZS, et al. Bone disease in multiple myeloma: biologic and clinical implications. Cells. Jul 27 2022;11(15).
2. American Cancer Society. Drug therapy for multiple myeloma. Updated August 15, 2023. Available at cancer.org.
3. The Multiple Myeloma Research Foundation. Treatments for multiple myeloma. Available at themmrf.org.
4. Mikulaki D, et al. Risk factors of infection in relapsed/refractory multiple myeloma patients treated with lenalidomide and dexamethasone (RD) regimen: real-life results of a large single-center study. J Clin Med. 2022 Oct;11(19):5908.
Patient Engagement
Boosting patient
resilience after relapse


Paid Advertiser
Paid Advertiser
“The earlier we can get social workers involved in addressing the needs of the individual patient, the better off they’ll be in the long run.”
—Kate Campion, DNP, AGACNP
One of the hard realities for patients with multiple myeloma (MM) is that the disease is incurable, and they almost certainly will experience relapse.1 What’s more, according to findings from a study based on data collected from interviews with 50 relapsed and/or refractory MM patients, for many of them, relapse had a greater negative impact on their emotional well-being than their initial diagnosis, with the news of their recurring symptoms bringing on feelings of hopelessness, devastation and resignation.2
Kate Campion, DNP, AGACNP, a nurse practitioner in the hematologic malignancies department at the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, has seen this in her own practice, explaining that for the patient, “A diagnosis of cancer of any type is overwhelming—many things are happening quickly, and patients often don’t have time to process everything. With time, information and a multidisciplinary team approach, patients and their families feel supported and come to a better understanding of their disease. They get into a routine—but the routine changes at the time of relapse, which can be disconcerting.”
This can have many consequences. For example, one study estimated that about 25% of patients with MM are diagnosed with psychological distress and symptoms of depression.3 Among the burdens outlined by the authors: failed hopes and expectations of a cure, loss of emotional and physical stability and worries about burdening loved ones, among others. “It’s not just the health of these patients—you have to take into consideration the broad impacts that this diagnosis has on all aspects of their life: financial implications of paying for treatment, loss of income for themselves and their caregivers in time away from work to receive treatment, as well as the impact that the diagnosis has on their hopes, dreams and future plans,” says Campion.
The study authors also surveyed physicians about their patients’ distress and found that, while the majority of hematologists were aware of the emotional burdens related to relapse, many did not feel confident or that they had the time or tools to discuss these issues.3
Fortunately, there are simple steps you can take to improve their ability to not only cope but also thrive. Campion has seen the effects of helping her patients first-hand and offers these suggestions for providing psychosocial support after relapse.
Ask questions and listen with compassion
For Campion, one of the most important things a healthcare provider can do for a patient who is processing the information that they have relapsed is to offer a path forward and be attuned to their reaction. So in addition to offering treatment options, ask patients how they’re doing emotionally and normalize their reactions. Campion offers this example: “If I’m seeing anxiety, I state, ‘What I’m hearing is you’re anxious. I want you to know this is normal for patients in this situation, and you are not alone.’ ”
She adds, “It’s important to remind them that this is a lifelong partnership. We’re here to provide guidance, answer questions and help them and their family and caregivers. We assure them that we will always be forthcoming and honest and will ensure that we are following their wishes. This can open the door for the bigger, scarier conversations.”
For clinicians who are hesitant to broach the topic, Campion’s advice is to jump in. “Practice makes perfect. It can be uncomfortable at first, but the earlier you start those conversations, the more routine it will become,” she says.
“It’s important to remind them that this is a lifelong partnership. We’re here to provide guidance, answer questions and help them and their family and caregivers.”
—Kate Campion, DNP, AGACNP
Create a support team
It’s crucial for physicians to help construct a healthcare team for each patient to address the impact of the condition from all angles, including the support of a clinical nurse specialist as well as management of pain and psychologic support, ideally from someone specializing in oncology.
Campion emphasizes the importance of adding a social worker to the mix, who can help patients with the psychosocial aspects of their cancer, such as preparing advanced directives and finding financial support for those who need assistance. She recommends engaging these team members in a patient’s care as soon as possible. “The earlier we can get social workers involved in addressing the needs of the individual patient, the better off they’ll be in the long run,” she says.
Guard against isolation and depression
Because isolation can have a negative impact on a patient’s frame of mind, Campion suggests asking questions such as, “Who do you have in your life to talk to? What is important to you? Where do you find strength and support?” and, when needed, “Have you been connected with a counselor?” She also recommends directing them to support groups to help them build relationships with other patients.
One thing she pays special attention to: “When I hear that they’re not seeing people as much, that’s a red flag that they may be withdrawing from relationships,” says Campion, adding that such behavior “can raise a concern for depression, which is something many of our patients experience.”
Complicating matters is that when COVID numbers climb, patients may choose to limit social interaction for health reasons. In those cases, she says, “I try to encourage them to find alternative ways to get together if they don’t feel like going out—maybe invite somebody over for coffee or just maintain the relationship by answering the phone when people call.”
Help them devise a practical plan
For patients who have relapsed and are concerned about burdening family and caregivers, Campion’s advice is to make a plan. Items to consider: deciding who among their family and friends to pull into their care, having a game plan for getting to and from appointments and, if they are working, speaking to their HR department about what to do if they need to employ the Family Medical Leave Act (which allows for missing work intermittently).
She also suggests ensuring that patients implement advance directives for end-of-life care early in the course of their disease if they have not already done so. While a healthcare provider may be hesitant to make this recommendation, she says it can actually help some patients feel more in control knowing that they’ve laid out their wishes. It also answers some of the unknowns when patients think about the worst-case scenario, which can add to their overall stress, and help alleviate worries about burdening others with “big decisions.” Says Campion, “I feel like that’s one of the best gifts we can give to our families.”
Provide education throughout their journey
Campion has found one of the best ways to address a patient’s anxiety after a relapse is with education—but with the right sources. “When patients go home and read everything they can, it tends to be overwhelming and just adds to the confusion,” she says. “I like to help direct them to a couple of places that have good information.” One of her favorites is the International Myeloma Foundation (myeloma.org), where patients can find information on treatments, new medications and clinical trials, and how to connect with other patients.
She also takes extra time to go over the specifics. “I’m frequently re-educating on the course of the disease and their specific disease so they understand what labs we’re following and there are no surprises,” she explains. She also makes sure to talk through what a future relapse may look like so they’re less likely to be caught off-guard.
Encourage healthy outlets
Research suggests that stress relief is important not only for emotional resiliency but also for enhancing immunity, including in people with chronic disease.4 That’s why Campion encourages patients to continue doing things they enjoy that bring them peace, such as meditation, religious activities and yoga. In general, she also advises her patients to leave the house for a walk “to be outside in the sunshine and change your view for a couple of minutes.” She says walking can help shift a patient’s frame of mind and encourage those with low energy levels to stay active, which in turn may help alleviate their fatigue.
—by Beth Shapouri
References
1. Ahmed A, et al. Relapsed and refractory multiple myeloma. StatPearls [Internet]. Updated June 8, 2023.
2. Hulin C, et al. Living with the burden of relapse in multiple myeloma from the patient and physician perspective. Leuk Res. 2017 Aug;59:75-84.
3. Noonan K, et al. A focus on relapsed multiple myeloma. J Adv Pract Oncol. 2022 Jul;13(suppl 4):15-21.
4. Morey JN, et al. Current directions in stress and human immune function. Curr Opin Psychol. 2015 Oct 1;5:13-17.
5. Glenn DG. Behavioral risk factors: a guide for oncology nurses counseling patients. Clin J Oncol Nurs. 2020;24(5):9-18.
Case Study


Paid Advertiser
Paid Advertiser
PATIENT: JOHN, 74, WAS DIAGNOSED WITH MM IN 2018. HIS MEDICAL HISTORY WAS NOTABLE FOR MI WITH STENTING, CAD, HYPERTENSION, PREDIABETES AND CHRONIC SUPPURATIVE OTITIS MEDIA WITH HEARING LOSS.
“For high-risk patients who relapse, using the most effective therapy early is critical”


PHYSICIAN:
Patrick Hagen, MD, Associate Professor of Medicine, Division of Hematology & Oncology, Loyola University Medical Center, Maywood, IL
History:
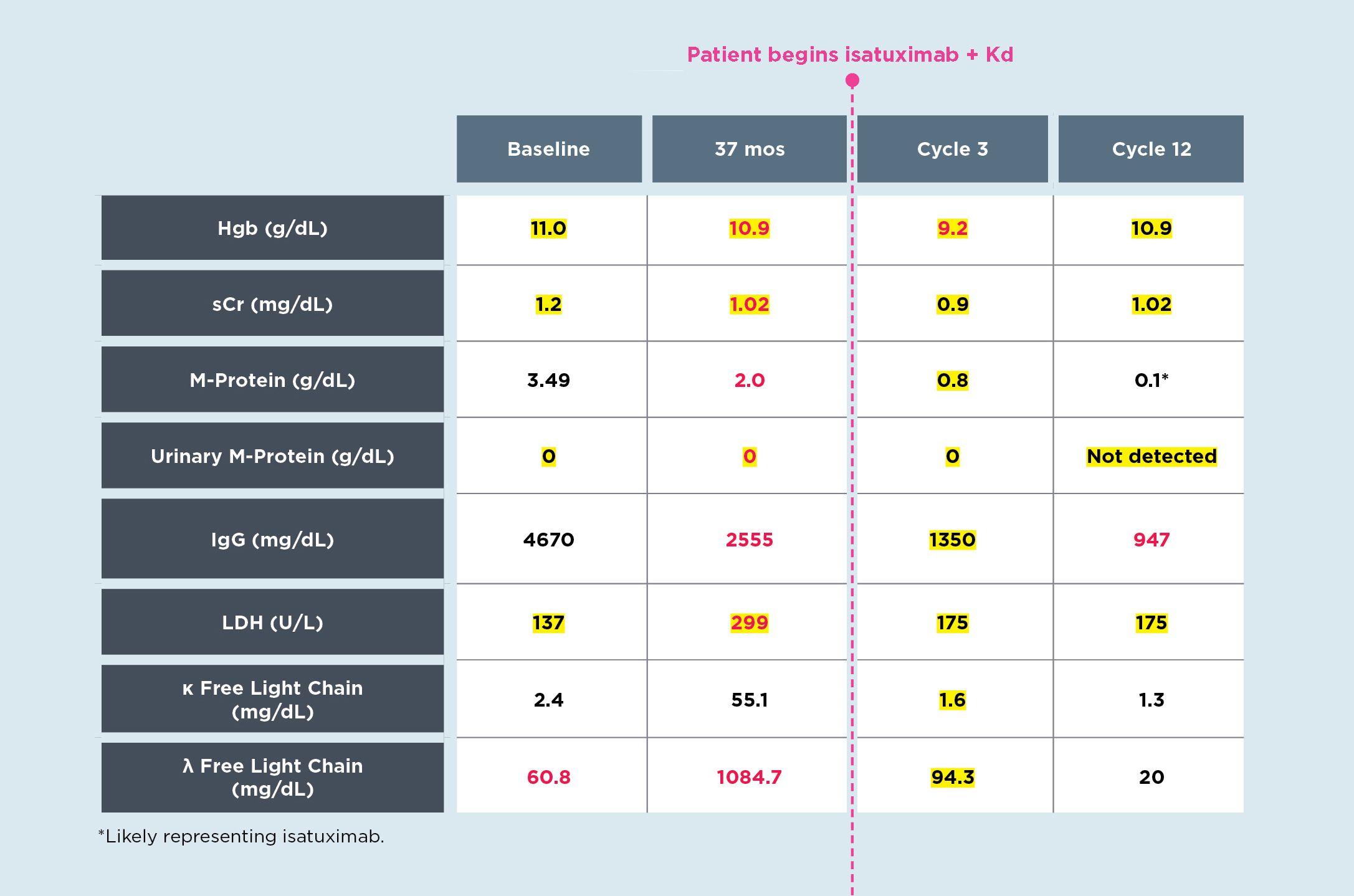
John presented to the hospital for persistent lower back and hip pain after a fall. Serum protein electrophoresis showed 3.49 g/dL of monoclonal protein, at which time he was referred to me for evaluation. John, who was married with adult children, had led a sedentary lifestyle after retirement as a research chemist. He and his wife had previously enjoyed babysitting their two grandchildren every week, but John no longer had the energy. Initial lab findings indicated multiple myeloma (MM) and advanced skeletal imaging confirmed John had multiple lytic lesions. His bone marrow results showed a normocellular marrow with 37% lambda restricted plasma cells and a MM FISH panel showed gain 1q as well as gain of 5/5p, 9/9q and 15/15q. At diagnosis John was noted to have a 1q gain, which is a common genetic abnormality occurring in 40% of MM cases and is associated with inferior outcomes. Both NCCN guidelines and mSMART 3.0 guidelines include gain1q as a high-risk genetic abnormality. Yet despite the frequency and high risk, management of patients with gain1q is poorly defined. John and I discussed treatment, including potential adverse effects, and he was ready to start therapy immediately.
First-line therapy included bortezomib-lenalidomide-dexamethasone (initiated as seven 28-day cycles). John achieved a very good partial response (VGPR) to induction therapy, and he was put on weekly maintenance therapy while his otitis media was being addressed in anticipation of high-dose chemotherapy and stem cell transplantation, which he would subsequently undergo. Adjunct treatments included denosumab.
Unfortunately, after 37 months, John’s MM progressed: M-protein reappeared and lambda sFLC increased, with additional lab work and bone marrow results indicating progression. He also had worsening fatigue and increased bone pain. PET-CT scan showed new low-level involvement in his ribs, pelvis and proximal femur, with greatest uptake notable in the right iliac wing.
Initiating treatment:
John and I discussed second-line therapy. He was a good candidate for a regimen that included isatuximab. Recent data show that isatuximab, when used in combination with carfilzomib + dexamethasone or pomalidomide + dexamethasone, can significantly prolong progression-free survival in high-risk patients and, in particular, those with gain of 1q. Again, I counseled John on potential adverse effects before initiating treatment.
John started isatuximab + carfilzomib-dexamethasone (Kd). During cycle 1, his infusion time was decreased to 75 minutes at week 3 due to the absence of infusion-related reactions. Because of his chronic supporative otitis media, denosumab was discontinued due to concern for osteonecrosis. At cycle 3 follow-up, John’s labs showed partial response (see Table, column 3, below) and his fatigue and bone pained resolved.
At cycle 6 follow-up, John showed VGPR, and immunofixation electrophoresis showed IgG lambda M-protein. Bone marrow showed no clonal plasma cells, and John said he felt well. After cycle 12, John’s status remained the same (see Table, column 4, below), and he continues to feel well. John and his wife are grateful he has the energy again to enjoy their family as they look forward to the birth of their third grandchild.
Considerations:
While there has been significant advancement in treatments for MM, unmet needs remain. High-risk patients continue to have suboptimal outcomes including patients who are older, have high-risk chromosomal changes, have impaired kidney function, and those who are refractory to multiple drug classes.
In a subgroup analysis of the IKEMA trial, treatment with isatuximab + Kd after early relapse of MM resulted in median progression-free survival for approximately 42 months in a patient population enriched with high-risk genomics including gain of 1q. It is key to remember that after relapse, it’s critical to use the most efficacious treatment early rather than reserving it for third-line or later therapy in order to achieve the deepest and longest remissions. For high-risk patients like John, prioritizing a regimen with the highest long-term efficacy can improve outcomes and help them live as well as possible for as long as possible.

Q&A
Insight on managing relapsing multiple myeloma


Paid Advertiser
Paid Advertiser
OUR EXPERT:

Joseph Mikhael, MD, MEd, FRCPC, FACP, Chief Medical Officer, International Myeloma Foundation; Professor, Applied Cancer Research and Drug Discovery, Translational Genomics Research Institute (TGen), City of Hope Cancer Center; Adjunct Professor, College of Health Solutions, Arizona State University
Newer therapies with durable efficacy
Q: How is the treatment paradigm changing for MM—particularly, relapse after first-line therapy?
A: There has been a revolution in therapies for relapsed multiple myeloma (RMM). The first wave of this movement was in a series of phase 3 trials that explored multiple triplet combinations to provide deeper and more durable responses than had been seen before in relapsed myeloma. This has now resulted in multiple options for therapies combining agents from the three main classes of proteasome inhibitors, immunomodulatory agents and monoclonal antibodies. In addition, a fourth class of agents, XPO1 inhibitors, has been developed and now incorporated into early relapse triplet combinations.
The second major wave of relapsed therapies has been focused on later relapse and has been in the realm of immunotherapy with both chimeric antigen receptor (CAR) T-cell therapy and bispecific antibodies. Indeed, two different CAR T-cell therapies have been approved in myeloma, both of which target the BCMA (B-cell maturation antigen) on the surface of the myeloma cell. These therapies literally tripled the response rate of traditional late-stage myeloma therapies with response rates in the 75% to 98% range. These deep and durable responses also have the advantage of CAR T-cell therapy being a “one and done” approach whereby we do not routinely give maintenance therapy after T-cells are reinfused. There have also been three bispecific antibodies approved for relapsed myeloma, two that target BCMA and one that targets the novel GPRC5D antigen on the myeloma cell. These therapies have a response rate of approximately 63% to 75%, at least doubling the rate of prior therapies (with the exception of CAR T-cell). Although they do require ongoing therapy, they do not need T-cell collection from the patient as with CAR T-cell therapies. Both CAR T-cell therapy and bispecific antibodies do come with the risks of CRS (cytokine release syndrome), neurologic toxicities and infections, but we are working toward minimizing their risks while optimizing their benefit.
Providing hope and support
Q: After a patient experiences a relapse, what psychosocial concerns do they commonly have and how do you counsel them?
A: This is such a critical question because at times, as providers, we can focus on the physiological and not fully consider the psychological concerns. And this becomes an even greater issue as our patients live longer with myeloma and more patients obtain very deep remissions. There are indeed many psychological concerns that arise in relapsed myeloma, but here are a few highlights of the most common ones.
Fear may well be the greatest worry—fear of relapse is real, especially as we know we essentially do not cure myeloma at this point. As a result, nearly all patients will indeed relapse, and we often cannot truly predict the timing of that relapse. Supporting our patients throughout their journey is essential, including being a source of hope to them. This is particularly pertinent as we do develop more and more therapies for patients.
Another great burden patients carry is financial. Often the disease results in loss of a job—this can be compounded by the high cost of treatment, often carried by the patient directly. Ensuring we provide financial resources and support is critical, including exploring all options for them while advocating for policies that reduce the financial burden on patients and their families.
Many of our myeloma patients also experience significant anxiety and distress. This can be related to the disease itself, the treatments given for it and the consequences of both. These issues cannot be underestimated as the disease, especially in relapse, is genuinely life-changing. Multiple interventions should be considered for these situations based on patient-specific needs. This should include regular engagement by the myeloma healthcare team and may also include mental health professionals.
Patients can also derive great benefit from meeting with other patients in the form of support groups. The International Myeloma Foundation (IMF) has over 150 support groups across the U.S. Patients can find a support group near them at https://www.myeloma.org/support-groups
Nondrug therapies
Q: What are nondrug interventions that can help manage MM symptoms?
A: One of the key phrases that guides me as I care for patients with myeloma is “we do not treat myeloma, we treat people.” This is a reminder of the critical nature of considering the whole patient as we take care of them. In doing so, we want to ensure we explore all options of therapy, both pharmacological and nonpharmacological. Myeloma, both the disease itself and its treatment, sadly comes with many symptoms that can significantly impair their quality of life, including fatigue, pain, neuropathy, weight loss, insomnia and many others.
Several nondrug interventions have been explored for each of these symptoms. Fatigue, which is very common in myeloma patients, can be addressed in multiple ways, such as staying active, optimizing sleep patterns, considering aromatherapy, practicing mindfulness and attempting deep breathing techniques. Similarly, many methods to reduce myeloma pain can be considered, such as gentle exercise, yoga, meditation, acupuncture, companionship, counseling, art/music therapy and dietary supplements (e.g., iron for anemia).
Neuropathy can be rather severe in myeloma, from the disease itself or from its therapy. Some of the nondrug strategies to treat neuropathy include dietary supplements (e.g., B vitamins and alpha lipoic acid), lotions/creams, essential oils, meditation and warm baths. For more information on these and other therapies, patients can visit the IMF website, https://www.myeloma.org/.
A bright future
Q: What are some promising advances on the horizon that could improve outcomes for RMM?
A: . In 25 years of myeloma care and research, I do not think there has been a more exciting time than the present for myeloma patients! In all areas of myeloma care, we have outstanding research ongoing to help patients live better, live longer and eventually, life without myeloma as we seek a cure. Some of these advances include:
Early detection and screening. Most patients diagnosed with myeloma are found after significant organ damage has occurred. We are exploring ways to detect myeloma earlier, with advanced techniques like mass spectrometry and the identification of circulating plasma cells in the peripheral blood.
Incorporating immunotherapies earlier in the disease course. As we see the incredible impact of CAR T-cell therapies and bispecific antibodies in heavily relapsed myeloma, we have tested these therapies in early relapse, as early as first relapse. The results of these large phase 3 trials are very exciting and will no doubt lead to the approval of these approaches in earlier relapse, if not even frontline therapy.
Addressing health disparities. Sadly, myeloma has tremendous health inequity in multiple groups, including Black individuals, who have twice the risk for MM and twice the mortality with the disease—which means Black patients have half the life expectancy with myeloma than white patients. This is being addressed, but has not been overcome yet, at multiple levels in the lay community, the healthcare system, the myeloma community, the government, industry and indeed the IMF through its M-Power project (for more details, visit https://mpower.myeloma.org/).
Clinical Minute:
Special thanks to our medical reviewers:
Carol Ann Huff, MD
Associate Professor of Oncology and Medical Director for the Johns Hopkins Kimmel Cancer Center
Joshua Richter, MD
Associate Professor, Icahn School of Medicine at Mount Sinai, and Director of Multiple Myeloma at the Blavatnik Family–Chelsea Medical Center
Maria Lissandrello, Senior Vice President, Editor-In-Chief; Lori Murray, Associate Vice President, Executive Editor; Lindsay Bosslett, Associate Vice President, Managing Editor; Joana Mangune, Senior Editor; Erica Kerber, Vice President, Creative Director; Jennifer Webber, Associate Vice President, Associate Creative Director; Ashley Pinck, Associate Art Director; Sarah Hartstein, Graphic Designer; Kimberly H. Vivas, Vice President, Production and Project Management; Jennie Macko, Senior Production and Project Manager
Dawn Vezirian, Vice President, Financial Planning and Analysis; Donna Arduini, Financial Controller; Tricia Tuozzo, Sales Account Manager; Augie Caruso, Executive Vice President, Sales & Key Accounts; Keith Sedlak, Executive Vice President, Chief Growth Officer; Howard Halligan, President, Chief Operating Officer; David M. Paragamian, Chief Executive Officer
Health Monitor Network is the leading clinical and patient education publisher in HCP offices, providing specialty patient guides, clinician updates and digital wallboards.
Health Monitor Network, 11 Philips Parkway, Montvale, NJ 07645; 201-391-1911; customerservice@healthmonitor.com.
©2023 Data Centrum Communications, Inc.
TCO23-CU-MM-1RAS